1061
Views & Citations61
Likes & Shares
Here we present a surgical case of intraoperative
aneurysm rupture. We want to highlight hyperaemic transformation of the
aneurysm wall during clipping as warning sign shortly preceding rupture.
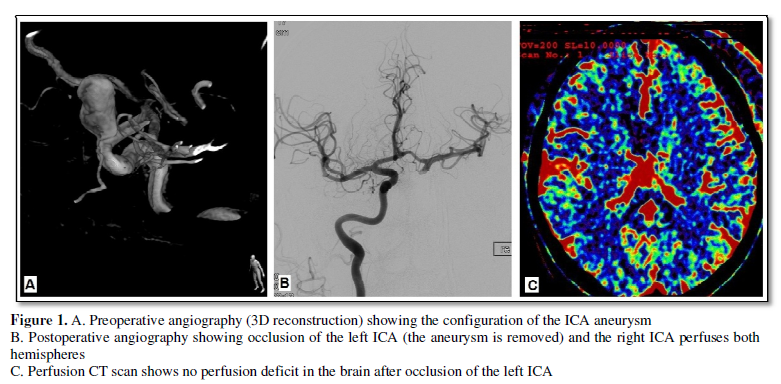
Clinical case: 61 year old male patient who complained of visual disturbances for months. Initial imaging with MRI revealed a giant aneurysm of the left internal carotid artery (ICA) immediately distal to the ophthalmic artery. Pre-operative angiography was performed and 3D reconstruction helped to plan the surgery. Figure 1A shows the angiography before surgery.
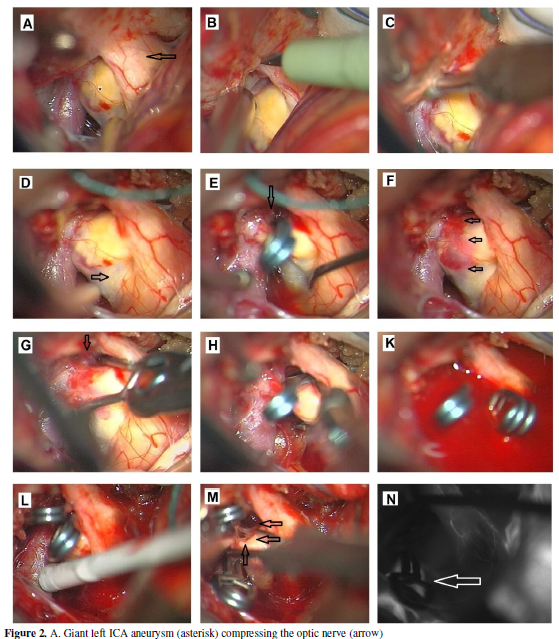
Surgery was performed through a pterional subfrontal approach. The most important surgical steps are shown in Figure 2. The aneurysm was highly atherosclerotic and impossible to be mobilized from the optic nerve. Next aclinoidectomy to achieve control of the ICA proximal to the ophthalmic artery was performed. Afterwards we dissected the aneurysm neck and applied a straight clip away sparing the ophthalmic artery. On slow release the clip slipped down and obliterated the ophthalmic artery. The clip was exchanged with a 45° angulated clip which still slipped down and obliterated the ophthalmic artery. We then decided to reapply a straight clip and to deflate the aneurysm. Because of important atherosclerotis deflation was almost without any effect. Nevertheless it was attempted to place a second clip over the first in order to remove the proximal clip and avoid obliteration of the ophthalmic artery. At that moment, we did not pay attention to the hyperaemic aneurysm wall which occurred after replacing the first clip. After little further manipulation of the aneurysm neck it ruptured. The ICA had to be clipped. As the aneurysm was ruptured at its neck and the wall extremely thin direct repair was impossible. There was no time left for an anastomosis at this point. Fortunately, there was excellent flow of the distal ICA perfused by the opposite ICA. The aneurysm was then trapped by clips. We removed parts of the aneurysm and decompressed the optic nerve. Immediately after surgery an angiography was performed which showed an excellent perfusion of both hemispheres from the opposite ICA (Figure 1B). Perfusion CT scan showed no perfusion deficit (Figure 1C).
The patient showed a delayed recovery. The blood
pressure was kept at 160 mmHg for the first 6 days. At day 7 the patient awoke.
No neurologic deficits could be seen. Obliteration of the ophthalmic artery had
no consequence. The visual disturbance decreased.
SUMMARY
There are some important points in this case:
- Atheromatous
aneurysms tend to rupture close to the neck
- A hypaeremic
transformation of the vessel wall is a warning sign of imminent rupture
- In case of
rupture of para-ophthalmic aneurysms the surgeon has to be prepared to
perform a bypass unless sufficient
distal perfusion is achieved by collateral flow Even with a “good”
aneurysm neck a safe proximal
control is mandatory
We would
like to discuss how other vascular neurosurgeons would have proceeded.
QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Rheumatology Research (ISSN:2641-6999)
- International Journal of Medical and Clinical Imaging (ISSN:2573-1084)
- Journal of Nursing and Occupational Health (ISSN: 2640-0845)
- International Journal of Diabetes (ISSN: 2644-3031)
- Advance Research on Endocrinology and Metabolism (ISSN: 2689-8209)
- Journal of Cancer Science and Treatment (ISSN:2641-7472)
- International Journal of Radiography Imaging & Radiation Therapy (ISSN:2642-0392)


